



The “timing” of treatment: a controversy
 One of the most controversial subjects in orthodontics is the ideal time to begin an orthodontic treatment for various problems encountered in growing patients. In most cases, the main concern is the benefit of treatment at an early stage of mixed dentition in comparison with another treatment that would be started in the late mixed dentition stage or in permanent dentition. One reason for this controversy is that the “cost” for early treatment is only part of a two-phase protocol. The first phase usually involves 6 to 12 months of active treatment with the intention of changing the dentoskeletal relationship between the jaws and the second phase is the “finishing” process after the eruption of permanent teeth. Thus, the analysis of risks versus benefits becomes inevitable. Do benefits of early intervention justify the cost and duration of a two-phase treatment? Some “classic” orthodontic studies have tried to answer these questions and some will be described below.
One of the most controversial subjects in orthodontics is the ideal time to begin an orthodontic treatment for various problems encountered in growing patients. In most cases, the main concern is the benefit of treatment at an early stage of mixed dentition in comparison with another treatment that would be started in the late mixed dentition stage or in permanent dentition. One reason for this controversy is that the “cost” for early treatment is only part of a two-phase protocol. The first phase usually involves 6 to 12 months of active treatment with the intention of changing the dentoskeletal relationship between the jaws and the second phase is the “finishing” process after the eruption of permanent teeth. Thus, the analysis of risks versus benefits becomes inevitable. Do benefits of early intervention justify the cost and duration of a two-phase treatment? Some “classic” orthodontic studies have tried to answer these questions and some will be described below.
Can we grow a mandible orthodontically?
Comparison of normal mandibular growth, a temporary growth acceleration with orthodontic treatment and theoretical stimulation of mandibular growth.
When a malocclusion includes mandibular rétrognathia as in Class II cases (short mandible, receding chin, significant horizontal gap between the front teeth (overjet)), mandibular growth is an important and essential element for correcting such a malocclusion. The lack of growth may mean that an orthognathic surgery is necessary to balance the jaws. Thus, it is important to begin the treatment of “Class II” cases at the perfect time to take full advantage of the growth potential of each patient. But does this mean that treatment should be started as soon as possible in a preliminary phase (phase 1) to get the most out of therapy? Is there an advantage to treat a patient with a significant Class II malocclusion with a two-phase treatment (the first during the mixed dentition phase and the second during adolescence)?
 The orthodontic literature includes hundreds of studies describing various devices that aim at modifying mandibular growth beyond what would be normal growth. Most of these devices are functional devices (also called myofunctional) which bring the mandible in a more advanced position during growth. The short-term effects of these devices have been summarized in a recent meta-analysis that concluded that:
The orthodontic literature includes hundreds of studies describing various devices that aim at modifying mandibular growth beyond what would be normal growth. Most of these devices are functional devices (also called myofunctional) which bring the mandible in a more advanced position during growth. The short-term effects of these devices have been summarized in a recent meta-analysis that concluded that:
- functional devices can accelerate the rate of anterior (forward) mandibular growth before and during adolescence,
- there is a retaining effect on the upper maxillary growth,
- a significant portion of the correction of Class II malocclusions is the result of dentoalveolar changes rather than actual skeletal changes in the jaw relationship.(1)
In order for a first phase of orthodontic treatment to provide a real benefit to the patient compared to a treatment performed in two separate phases, it would have to:
- provide more growth than what would result from normal mandibular growth and
- result that persists over time of this additional gain growth.
However, it appears that the first point is possible, but the gains obtained during a first phase of treatment of a Class II malocclusion are only temporary and do not provide any real advantage over a treatment done in two distinct phases.
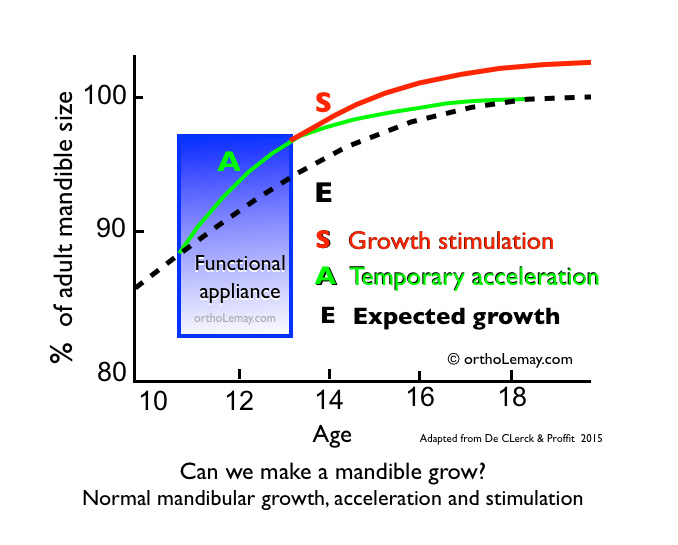
- This illustration shows the difference between the acceleration of mandibular growth (curve A in green), as it can be obtained with myofunctional or functional devices, and an actual stimulation of mandibular growth (S curve in red). Scientific evidence demonstrates that mandibular growth following the acceleration period is actually slower than normal growth that should be expected without any treatment or procedure (N curve in black) so that the total effect at the end of mandibular growth is minimal or null.(2)
- If growth stimulation using functional devices actually occurred, the growth curve in green would follow the red curve to the end of growth.

- Will the acceleration of mandibular growth during adolescence lead to bigger or longer mandible at the end of the growing period? The possibilities are illustrated in the following diagram. The conclusion is that the growth acceleration period is followed by a decrease in growth afterward. So, if there is a long-term increase in the size of the mandible, it is very small. Sometimes, the changes may be statistically significant and sometimes they are not, but the scientific evidence does not support the idea that we can “grow mandibles” orthodontically.
- The ideal timeframe to undertake a therapy to modify mandibular growth remains a subject of controversy in orthodontics, although several clinical studies come to the same conclusion: treatments performed in 2 phases and started before the growth spurt in adolescence are not more effective than one-phase treatments started during adolescence.(3)
- The main indication for treating a pre-teenager with a lower jaw that is too far back (mandibular retrognathia) is more a psychological indication for a child with psychosocial problems caused by the comments, teasing and harassment about his teeth that are too advanced and unesthetic rather than the presence of a severe malocclusion.
- Treating young children at first, then following with a second phase of treatment in early adolescence, appears to significantly reduce the incidence of new dental trauma to the incisors when compared to a one-phase treatment in early adolescence. However, this data should be interpreted with caution because of the high degree of uncertainty. So there is no other benefits to perform a two-phase treatment instead of only one phase in early adolescence.(4)
In 1995 Gianelly found that 90% of all orthodontic problems could be treated with a single phase treatment without undergoing a first phase, but 10% of patients who had crossbites causing functional movements of the mandible and some kinds of Class III malocclusions could benefit from immediate action to correct the problem.(5)
However, it would be good to clarify that in some severe cases, a real psychological advantage can be obtained by early intervention, but for growth and the end result, studies prove beyond any doubt that we cannot stimulate mandibular growth beyond the growth potential inherent to each person.
In summary…
What does the orthodontic literature say?
 Several orthodontic studies have demonstrated that we cannot differentiate, in adolescence, Class II patients who had a first phase of treatment at an early age (preliminary treatment) from those who have had a treatment performed in only one phase later on. Orthodontic and occlusal results were similar and the conclusion was that it was not indicated to perform a first phase of treatment.
Several orthodontic studies have demonstrated that we cannot differentiate, in adolescence, Class II patients who had a first phase of treatment at an early age (preliminary treatment) from those who have had a treatment performed in only one phase later on. Orthodontic and occlusal results were similar and the conclusion was that it was not indicated to perform a first phase of treatment.
What do orthodontists think of this?
Another study compared orthodontists’ perception on the impact of a first phase of an orthodontic treatment done in mixed dentition on the need to perform a following second phase of treatment for Class II cases (mandibular retrognathia). Orthodontists did not know which treatment modality had been made on the individuals they were evaluating (one-phase or two-phase treatment).
They concluded that they did not consider a first phase of treatment as a way to prevent the need to perform a second phase of treatment and that a first phase of treatment offered no real advantage with respect to the need to use extractions or skeletal corrections during the second phase. However, early treatments can reduce the difficulty and priority of the second phase.(6)
- Therefore, THE QUESTION is not whether early treatment of Class II or mandibular retrognathia cases works at an early age, because we know that some interventions may be beneficial, but rather to determine if there is a benefit to the patient to intervene in mixed dentition since the benefits obtained will be inseparable from those obtained by a single-phase treatment started later and this is amply illustrated and documented in the orthodontic literature. This is not because it is possible to do them that such interventions must be made at an early age.

- To understand well what aspects of a skeletal problem can benefit from a first phase of treatment, malocclusions must be evaluated in 3D (three dimensions). Mandibular defects (length) rarely benefit from a first phase of treatment, while the treatment of transverse (width) and vertical (height) problems can offer real benefits to the patient during a first phase performed at an early age, although most of them could also be treated in a single phase a little later.
- Note that this conclusion on early treatment of malocclusions with a skeletal component applies only to mandibular defects (mandibular retrognathias – Class II malocclusions) and cannot be applied to all problems encountered in mixed dentition.
- ➡ To see examples of Class II cases treated in orthodontics during a one-phase treatment in adolescence.
- There are several skeletal conditions affecting the two other dimensions that can be treated at an early age with significant benefits such as:
- transverse maxillary deficiencies (posterior crossbite, “width” problems of the jaws) that can be treated using rapid maxillary expansion or
- sagittal maxillary deficiencies, whether caused by mandibular prognathism (advanced mandible) or an upper jaw that is too far back, two problems causing Class III malocclusions.
- ➡ To see examples of such corrections, see the section on rapid maxillary expansion and facemask.
- In addition, several conditions require early intervention, such as selective extractions and several preventive and interceptive treatments.
When does growth need to stop before intervening?
- The previous discussion is about the timely moment and benefits of treating a specific skeletal problem (mandibular retrognathia) in one or two phases in patients still having good potential. Regardless of the approach chosen by the practitioner, the presence of growth is a vital asset to treat more easily a skeletal deficiency problem (transverse or sagittal). Even the most severe Class II cases can benefit from being treated in adolescence during the patient’s growth spurt.
- However, when there is excessive growth, as in prognathism where the mandible is too long or too advanced compared to the upper maxilla (Class III cases), depending on the severity of the imbalance, it may be appropriate to wait until growth stops to intervene. If a teenager already shows an extreme imbalance, it would be risky to treat him while knowing that the residual growth can cause a new imbalance at the end of treatment. In such cases, it is best to wait until there is no more growth and treat the malocclusion in a single phase which includes an orthognathic surgery (see the case below for an example).
- However, smaller imbalances may be treated even if the patient’s growth is not yet finished, while keeping in mind that that there is a possibility that the remaining growth affects the results and stability of the corrections.

Given the gravity or severity of this Class III malocclusion already present in this teenager and, since it is determined at that time that an orthognathic surgery will be necessary to correct the imbalance of the jaws, it was better to wait until there was no more growth to intervene with an “ortho-surgery” approach and thus prevent the remaining growth from causing a relapse after the orthodontic treatment.
References:
1- Vaid NR, Doshi VM, Vandekar MJ. Class II treatment with func- tional appliances: a meta-analysis of short-term treatment effects. Semin Orthod 2014;20:324-38.
2- Proffit WR, Fields HW Jr, Sarver DM. Contemporary orthodontics. 5th ed. Philadelphia: Elsevier; 2013.
3- Thiruvenkatachari B, Harrison JE, Worthington HV, O’Brien KD. Orthodontic treatment for prominent upper front teeth (Class II malocclusion) in children. Cochrane Database Syst Rev 2013; (11):CD003452.
4- Badri Thiruvenkatachari, Jayne Harrison, Helen Worthington, and Kevin O’Briend, Early orthodontic treatment for Class II malocclusion reduces the chance of incisal trauma: Results of a Cochrane systematic review. Am J Orthod Dentofacia Orthop 2015;148:47-59
5- Giannelly, AA , One-phase versus two-phase treatment –American Journal of Orthodontics and Dentofacial Orthopedics November 1995 Volume 108, Issue 5, Pages 556–559
| :Updated: 2016-08-05 at 17:19:50 © Jules E. Lemay, www.ortholemay.com |