
 (8 votes, moyenne: 4.63 sur 5)
(8 votes, moyenne: 4.63 sur 5)


Serial extractions are a preventive and interceptive procedure that consists of strategically extracting certain temporary teeth in situations where there is a severe lack of space in the mouth and/or the eruption path of the permanent teeth is abnormal. Like a compass, this procedure aims at orienting the teeth to facilitate their eruption.
- This procedure allows some redistribution of space to permanent teeth that attempt to come out but which, because of a lack of space, have an abnormal eruption.
- It is important to understand that these extractions do not create space. The space already available is used (redistributed) to facilitate the eruption of teeth.
- Extractions may be necessary in each jaw and usually span over several years.

- A panoramic radiograph and a clinical examination around 7-8 years of age will allow the orthodontist to evaluate the available space for the developing permanent teeth, as well as their eruption path, so an early evaluation is important.
- If a significant lack of space or other problems are visible on the radiograph, we will recommend that your dentist proceeds with the extraction of specific temporary teeth.
- Following the extractions, the child will then be evaluated by Dr Lemay every 12 to 18 months to follow the evolution of tooth eruption. Depending on the case, other extractions of temporary teeth may be recommended.
- The follow-up will be done yearly up until the permanent teeth erupt. Appropriate recommendations on indications to correct the malocclusion (orthodontic treatment) will then be made.
- These procedures being indicated only when there is a severe lack of space, one needs to expect that, despite the extractions of temporary teeth, not all permanent teeth will erupt in a normal or ideal position.
- Most of the time, orthodontic corrections are still necessary to obtain an esthetic and functional occlusion.
- Growth alone usually does not help a severe space deficiency, because it occurs mostly at the back of the jaw rather than at the front or on the sides where space is most necessary.

Radiograph showing a different eruption pattern for both permanent upper canines that are still in the gingiva. (A) On the right side, the canine has an eruption path parallel to that of the lateral incisor which remains straight (yellow arrows). (C) On the opposite side, the canine collides with the lateral incisor that tilts backward and tips forward (blue arrows). The serial extraction of temporary teeth can help influence the eruption path and guide the left canine for this 9.9-year-old boy.

The panoramic radiograph of this 10-year-old girl allows the detection of several eruption problems (circled) for which an intervention is indicated. The extraction of temporary teeth can help change the abnormal eruption path of permanent teeth.
| The permanent canines often need help! Serial extractions make it possible to influence the eruption path of the permanent teeth and particularly the permanent upper canines which are often tilted forward. The example on the opposite side shows how the extraction of two temporary teeth allowed one canine (red dotted line) to upright and head toward where it must erupt in the arch. Even if this intervention helps the eruption of the canine, there is still a lot of space missing to allow this tooth to erupt normally and orthodontic corrections will still be necessary later on to correct this situation and obtain a normal occlusion. To know more on impacted and ectopic canines. |
 (A) Canine tilted toward the lateral incisor (dotted line). The temporary teeth indicated by a (*) will be extracted. (B) A little more than one year after the extractions, there is a significant improvement of the eruption path of the permanent canine. |

When there is a severe lack of space for the eruption of the permanent teeth, temporary teeth can be extracted (X) to help the permanent teeth erupt (arrows).

Significant crowding in both arches in a 9-year-old young girl. Serial extractions of the temporary canines (indicated by asterisks *) will relieve the anterior crowding and help the eruption problems affecting the other permanent teeth.
Why don’t temporary teeth fall out by themselves?
People frequently ask us this question when we recommend serial extractions.
The reason to extract temporary teeth during an interceptive phase in orthodontics is not that these teeth do “not want to fall out” by themselves, but rather we want to extract them before they exfoliate (shed) by themselves because it could still take several months to more than one year before this would happen naturally and during that time, the eruption problems persist and can often worsen.
What would happen if the selected teeth were not extracted?
Teeth to extract serially or early would all end up shedding by themselves eventually. The problem is that it would occur too late to modify the eruption path of permanent teeth that will replace them and which already show an abnormal and potentially problematic eruption path. The additional delay may cause several eruption problems and worsen the developing malocclusion.
Space that is worth gold!
Robbing Peter to pay Paul!
This metaphor clearly illustrates what we try to do with serial extractions, that is stealing some space from someone (temporary teeth) to give back to someone else (permanent teeth).
- Temporary teeth are “sacrificed” to create space that will be useful for the eruption of the permanent teeth by attempting to “redirect” their eruption.
- The dental arch only has a definite and limited amount of available space to accommodate the teeth. Even though growth increases the dimension and volume of the jaws during a certain period, it ends relatively early so that at around 6-8 years of age, and depending on the speed at which the child is developing, certain areas of the jaws have stopped growing to accommodate the future teeth.
- We thus use serial extractions to transfer the space of certain (temporary) teeth to others (permanent teeth) that need it more and earlier.
- Serial extractions do not “create” space, but rather redistribute the space already available to teeth that try to erupt.
To find out more on jaw growth and development.
Will I avoid an orthodontic treatment with these extractions?
NO, absolutely not!
- You can choose that your child does not undergo an orthodontic treatment later on if you wish, but it is practically certain that there will still be several indications to envision orthodontic corrections if you wish that your child’s dentition be functional and esthetic.
- You must remember that the main indication to recommend serial extractions is a situation where there is a severe lack of space and significant eruption problems, so simply extracting temporary teeth will not make it possible to fix all the problems.
- For instance:
- If the jaws are shifted, too narrow, asymmetrical, etc., extracting temporary teeth will not change any of these problems.
- If upper teeth are very prominent (sticking out), if they show an excessive overbite, if they have significant rotations or malpositions, etc., extractions will have no or very little effect on that.
- If an anterior open bite is present, if a tongue problem exists, or other conditions related to musculature, serial extractions will have little effect on these problems.
Although this procedure does not guarantee that permanent teeth will come out adequately, most of the time, it still contributes to minimizing eruption problems and will often facilitate orthodontic corrections that will be indicated when the permanent teeth have erupted.
Dental radiographs: an essential diagnostic help
- To help the orthodontist with the supervision of the eruption of teeth, panoramic radiographs are essential to make a good diagnosis and make recommendations that aim at intercepting developing problems and minimizing their consequences.

- General dentists regularly take small X-rays that are placed in the patient’s mouth to be exposed (retroalveolar, periapical and bite-wings). These X-rays only cover a few teeth, but with more precision and details than a large panoramic radiograph. They are indicated when we are trying to identify small lesions, cavities, bone defects, etc.
- In orthodontics, we mainly use panoramic radiographs that make it possible to have a “global view” of the situation (teeth erupted in the mouth, developing unerupted teeth, jaw joints, etc.), but with less details. However the new digital radiographic machine that we now use offers image quality and resolution that is better than most small film radiographs.
- If indicated, small radiographs may be taken to obtain additional diagnostic information on a particular area (an impacted canine for instance) but this is rarely necessary with the advent of digital radiography.
- Moreover, in 2012, we acquired a radiographic machine that allows us to take “scans” or 3D radiographs (cone beam computed tomography (CBCT)) that make it possible to obtain images that help us in the diagnosis of particular problems like impacted teeth (canines and others). We rarely have to take such X-rays in children but we could if required. To know more on this type of 3D radiographs and see examples
- Radiographs are for us a kind of “crystal ball” that allows us to “predict the future” of dental eruption.
To know how the evaluation of the position of canines on panoramic radiographs at an early age can allow us to intervene early and maximize the chances that these teeth erupt the best way possible, follow this link.
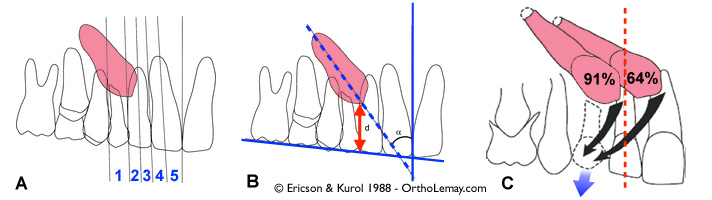
Prediction methods for canine impaction developed by Ericson and Kurol by evaluating (A) the position of the canine compared to zones defined on a panoramic radiograph, and (B) the distance of the tip of the canine compared to an (occlusal) plane. (C) Success rate of canine autoeruption if the temporary canine is extracted depending on its position compared to a bisector traced on the lateral incisor.

A real case!

Radiographs make it possible to locate and identify the presence of impacted teeth as shown in this example. (A) This young patient complained about a “bump in the palate” (indicated by the arrows). (B, C) In the mouth, the permanent upper left canine is missing (arrow) although the parents believed that it was extracted! (D) The X-ray confirms the presence of an impacted canine.
➡ To know more on dental radiographs.