



The “classical” option or conventional approach to treat anterior open bites with a skeletal component (vertical malposition of the jaws) requires a surgical intervention to “intrude” the posterior area of the upper jaw (superior repositioning) and allow an autorotation of the lower jaw which contributes to closing the open bite. The advent of mini-screws or temporary anchorage devices (TADs) now allows us to obtain similar results by intruding upper posterior teeth and avoiding a surgical procedure (jaw surgery). Intrusion with TADs has been proven to be a less invasive way to correct moderate skeletal open bites while minimizing the costs and risks associated with orthognathic surgery.
The following illustrations show different orthodontic anchorage appliances (splints) which can be used with TADs for the treatment of anterior skeletal open bites. In such cases, the posterior teeth are often the only ones contacting one another during mandibular closure thus creating an anterior open bite.
To illustrate this type of treatment and show different orthodontic appliances that can be used in the correction of skeletal anterior open bites using mini- screws and temporary anchorage, we obtained permission from Dr. Nicole R. Scheffler, orthodontist in Boone, North Carolina, to use some photos of a clinical case that she treated and was published in a scientific orthodontic journal. (1)

Dr. Scheffler is a pioneer in the use of miniscrews for temporary anchorage and she developed treatment protocols to treat skeletal open bites using these appliances. The images on this page were used with her permission.
There are two main ways to reduce an open bite by orthodontic movement;
- by intruding (moving up) the upper posterior teeth that are in contact during jaw closure,
- by erupting or extruding (moving down) the upper anterior teeth to bring them closer together.
- A combination of these two types of movement can also be used.
The choice of movement will depend on several factors including the visibility of the anterior teeth when smiling. If the upper teeth are already very visible and there is gingival tissue showing (gummy smile) we will prefer intruding the posterior teeth rather than erupting the incisors which would increase the “gummy” aspect of the smile. Furthermore, major incisor extrusion tends to be less stable (higher potential for relaps) than posterior intrusion.
To learn more about orthodontic tooth movement (French text only).
The basic principle in the treatment of skeletal open bite using miniscrew anchorage is to apply a constant vertical force on the posterior teeth to progressively intrude them (move them up). The active force comes from super-elastic metal springs that are anchored to hooks on an intraoral anchorage orthodontic appliance (splint) bonded (glued) to the teeth and to the temporary miniscrews.
- The intra-oral anchorage appliance or splint, examples of which are illustrated in Figures 1 and 2 below, consists of a metal part that provides rigidity and stability to the device, some plastic (acrylic) and hooks to anchor the springs. The splint is bonded to the teeth with the same “glue” used for orthodontic brackets (adhesive composite). The patient cannot remove this appliance.
- The temporary anchorage devices (miniscrews) are placed in the vestibule of the mouth between the roots of the teeth. These miniscrews are removed at the end of treatment or during the retention phase. To learn more about miniscrew anchorage (in French only).
- Depending on the position of the miniscrews and hooks used to anchor the springs, force vectors can be created to act in a particular direction depending on the type of malocclusion to be corrected. The screw can be placed between the molars (Fig 1-A) and the hooks located farther back in order to obtain mainly some molar intrusion when these teeth are the only ones in vertical contact with the opposing teeth. The screw can also be placed between a premolar and a molar (Fig 1-B) when there is contact between the premolars and molars and the springs can be anchored on hooks positioned farther anteriorly on the splint
- The superelastic alloy (nickel titanium) springs are attached, 2 on each side, on the splint hooks and the miniscrews and produce a force of 150 g each. This alloy allows the springs to generate and deliver a uniform and continuous force and, therefore, they do not need to be changed (or rarely). Their attachment points (choice of hooks and position of miniscrews) determine the direction of action of the force (Fig 1 A and B).
- Some types of splints may also require the use of miniscrews in the middle of the palace to attach the springs (Fig 2 – B and C).
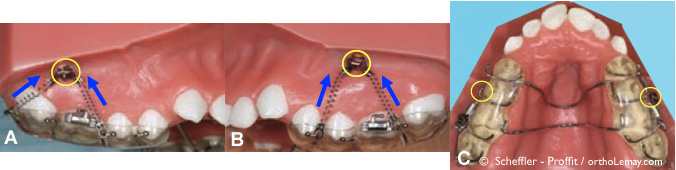
Fig. 1 – Examples of miniscrews (yellow circles) used to anchor springs aimed at intruding (arrows) the posterior teeth and help to correct a skeletal open bite. The springs are also attached to a fixed intraoral appliance (splint).

Fig. 2 (A, B, C) – Occlusal view of three types of appliances used with miniscrews for posterior teeth intrusion. (B) This type of device can also exert an anterior traction on the anterior maxillary teeth (arrows) and is used to treat cases of anterior open bite requiring also the correction of a moderate to severe Class 2 component. Four 150 g springs are attached to the palatal miniscrews. (C) If the open bite is accompanied by a moderate to severe Class 3 malocclusion, this device can be used. Two 250 g springs are attached to a miniscrew in the middle of the palace.

Fig (3) – Significant open bite and maxillary constriction (narrow jaws). Arrows indicate the necessary intrusion movement of the posterior teeth necessary to close the open bite. (D) Cephalometric radiograph showing the anterior gap between the teeth and contact between the posterior teeth.
Case characteristics and treatment progress
- This 13.9 year old adolescent has a significant anterior open bite characterized by vertical maxillary excess (skeletal problem) requiring posterior teeth intrusion.
- The dental arches are narrow (bilateral posterior crossbite) and have a lack of space (dental crowding).

Fig (4) – After 10 months of treatment, the teeth are aligned (correction of rotations and dental crowding) and miniscrews were placed. (A) Orthodontic braces in the mouth with miniscrews (yellow circles). Elastic springs are attached between the screws and the anchoring hooks on the splint bonded to teeth (visible in (B)). The splint and the miniscrews can be used without installation of the orthodontic brackets. When installing the splint, the anterior open bite will seem to increase because of the thickness of plastic (acrylic) between the teeth but this will correct itself as the intrusion of posterior teeth occur sand the open bite closes.
Open bite closure progresses at a rate of approximately 1 mm per month but the biggest amount closure of anterior open closure bite occurs during the first 2 months. The splint is kept in the mouth until about 1 to 2 mm of anterior vertical overlap (overbite) is obtained or until the lower arch has been leveled, which takes an average of ± 6 months depending on the severity of the vertical and transverse (width) imbalance. In this case, the device was removed after 6 months but the miniscrews were left there.
After splint removal miniscrews are tied to the orthodontic brackets with a steel ligature to help maintaining the correction (intrusion) obtained and prevent relapse leaving teeth “down”.
Note that, although an adjustment period of a few days is needed to get used to the splint, patients tolerate it very well. Practitioners like Dr. Scheffler who developed this approach, report that they never had to remove this type of appliance due to discomfort.

(A) After posterior intrusion, anterior open bite is closed and there are now contacts between the anterior teeth. Note that the miniscrews remain in the mouth because they will be used for retention. (B) Occlusal view; the splint has been removed because it no longer needed.

Retention – (A) At the end of the orthodontic treatment (20.5 months) the braces were removed but the miniscrews are left in place (arrows) to serve as anchorage for the removable retainer for a period of six months. After that, the screws are removed but the patient continues to wear the removable retainer indefinitely at night only. (B) A retention wire (bonded retainer) is used on the inner surface of the upper and lower incisors.
Retention
These special open bite cases require not only specific therapeutic approaches but different retention protocols to maximize the chances of having stable corrections. In the case of this girl, an upper removable retainer was used with;
- occlusal coverage (chewing surfaces of the back teeth) to retain the teeth,
- a tongue crib (wire fence) or screen to keep the tongue away from the anterior teeth,
- hooks for attaching the removable retainer to the miniscrews with elastics. It is worn this way for a period of at least six months.
To learn more about orthodontic retention and stability and to see other retainers used in open bite cases (French).

(A) Retention appliance with hooks and elastics (blue arrows) to the miniscrews (yellow circles) and an oral screen (red arrows) for containing the tongue. Different view of this appliance (C) where you can see the hooks for attaching the elastic (yellow arrows). (B) Similar retention appliance but without elastic hooks. Such a retainer can be worn after 6 months when the elastic are no longer necessary.

(A and B) 18 months after the end of treatment, the bite (occlusion) is stable and the open bite remains closed.

Face and smile of the 13 year old patient (A) before treatment, (B) after 10 months, when the miniscrews were placed, (C) 6 months later, (D) at the end of active treatment (bracket removal) after 20.5 months of treatment and (D) 18 months after the end of treatment.
(1) Miniscrew-Supported Posterior Intrusion for Treatment of Anterior Open Bite, Nicole R. Scheffler, DDS, MS – William R. Proffit, DDS, Phd, JCO VOl XLVIII Number 3 p. 158-168